IBD Literature Report
Coverage: July 26, 2026 - August 02, 2026
17
Papers This Week
4
Categories
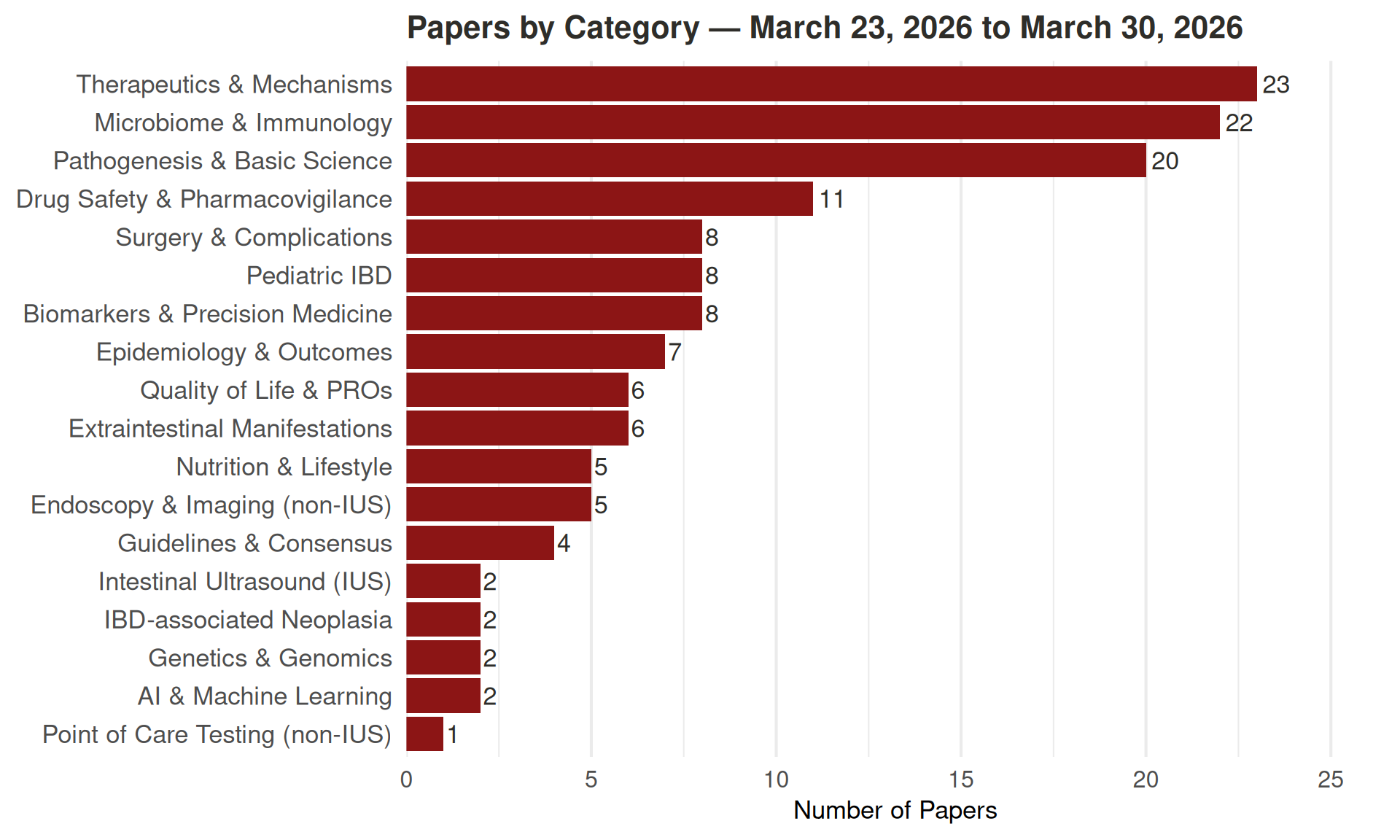
Papers by Category
Click a category to expand. Click a paper title to read its abstract.
Pathogenesis & Basic Science (11 papers)
MXRA7: A potential link between macrophage M1 polarization and epithelial Pyroptosis in ulcerative colitis. International immunopharmacology | 2026-07-31
Ulcerative colitis (UC) is a chronic inflammatory bowel disease characterized by persistent colorectal mucosal damage, in which colonic epithelial cell pyroptosis and imbalanced macrophage M1 polarization serve as core pathological features, yet their interaction mechanism remains elusive. Matrix remodeling-associated 7 (MXRA7) has been implicated in inflammatory immune responses and tissue repair, but its role in UC progression is still unclear. In this study, we performed bioinformatics and cell-cell communication analyses using the GSE214695 single-cell RNA sequencing dataset, collected clinical colonic tissues from UC patients, and established a dextran sulfate sodium (DSS)-induced mouse colitis model, complemented by in vitro cell co-culture, gene knockdown/overexpression and molecular biological assays. The results showed that pyroptosis levels, the degree of macrophage M1 polarization, and MXRA7 expression were all significantly upregulated in the colonic tissues of both UC patients and model mice. Mechanistically, macrophage M1 polarization can directly trigger colonic epithelial cell pyroptosis, whereas MXRA7 may, on the one hand, reduce macrophage M1 polarization by inhibiting the NF-κB signaling pathway, and on the other hand, alleviate epithelial cell pyroptosis induced by M1-polarized macrophages. Collectively, MXRA7 may attenuate colonic tissue damage through these dual regulatory mechanisms, thereby serving as a potential regulatory factor or therapeutic target in UC.
Zhu X, Tang K, Kang J, Cui N, Xiang H, Su W, He Y, Guo Y, Xiao M, Zhou Z
Regulation of Tph cell differentiation via farnesoid X receptor of dendritic cells in inflammatory bowel disease. Inflammation research : official journal of the European Histamine Research Society … [et al.] | 2026-07-31
Peripheral helper T cells represent a recently characterized subset of CD4+ T cells present in inflammatory bowel disease (IBD) patients. Bile acids act as signaling molecules in immune regulation. However, the role of bile acids in Tph cell differentiation remains unclear. Immunofluorescence staining was used to detect the presence of Tph cells in intestinal tissue samples; Wild-type (WT) and Fxr-/- mice were treated with or without the FXR agonist obeticholic acid (OCA) in dextran sulfate sodium (DSS)-induced acute colitis. The proportions of Tph cells and innate immune cells were analyzed by FACS. Bone marrow-derived dendritic cells (BMDCs) and naïve T cells of WT and Fxr-/- mice were sorted, differentiated and cultured in vitro to observe the regulatory effects of FXR on BMDCs function and Tph cell differentiation. Tph proportion was significantly elevated in inflamed intestinal tissues. OCA treatment increased the Tph cell proportion in the intestinal LP of WT mice. The proportion of dendritic cells (DCs) in the LP of Fxr-/- mice was significantly lower than WT mice after DSS-mediated colitis induction. FXR deficiency impaired the ability of BMDCs to induce Tph cell differentiation in vitro. CD11c and MHC-II expression levels were reduced in BMDCs from Fxr-/- mice upon stimulation with LPS. FXR deficiency activated the PPAR-γ signaling pathway and decreased IL-12 expression in BMDCs. Tph cell levels were elevated in inflamed intestinal tissues. FXR suppression in BMDCs was associated with activated PPAR-γ signaling; and with reduced DC maturation, IL-12 secretion, and Tph cell differentiation.
Hu Z, Liu M, Zhu C, Li N, Chen X, Da B, Li Y, Yu C
Enterococcus faecium MMX derived from traditional fermented mare’s milk alleviates colitis by modulating the LCN2-NLRP3 pyroptosis axis. Food & function | 2026-07-30
Ulcerative colitis (UC) is a relapsing inflammatory disorder of the intestine for which safe and effective therapeutic strategies are urgently needed. The present study aimed to isolate a novel probiotic strain from traditionally fermented mare’s milk (koumiss) and to characterise its molecular mechanism of action in alleviating UC through modulation of lipocalin-2 (LCN2) and the NLRP3 inflammasome-mediated pyroptosis pathway. We conducted a systematic investigation integrating microbiological characterisation, whole-genome sequencing, bioinformatic mining and a DSS-induced mouse model of colitis. The results suggested that the isolated Enterococcus faecium MMX strain exhibited no haemolytic activity, strong bile salt tolerance, absence of typical virulence factors, and carried certain resistance genes, while also harbouring multiple probiotic-associated functional genes. Multi-dataset machine learning analysis identified LCN2 as a key biomarker of UC, with its expression highly positively correlated with neutrophil infiltration. In vivo experiments revealed that E. faecium MMX significantly improved the disease activity index, restored the intestinal epithelial barrier (with recovery of E-cadherin expression), promoted goblet cell regeneration and markedly suppressed neutrophil infiltration. Mechanistically, E. faecium MMX treatment was associated with reduced total LCN2 expression in colonic tissue and a shift in its cellular source from a predominantly pro-inflammatory neutrophil-derived localisation to an epithelial cell-derived localisation, accompanied by suppression of the NF-κB pathway (as evidenced by reduced p-p65 levels), which correlated with inhibition of the NLRP3/cleaved-caspase-1/GSDMD-N/IL-1β pyroptosis signalling axis and diminishing the release of pro-inflammatory cytokines, including mature IL-1β and mature IL-18, as confirmed by ELISA and western blot analyses. Collectively, these findings suggest that E. faecium MMX may exert its anti-colitic effects by remodelling the host immune microenvironment, downregulating LCN2 and NF-κB signalling, and inhibiting pyroptosis, positioning it as a promising candidate for microbiota-based intervention in UC.
Ma M, Bao H, Li C, You F, Li Y, Zhang H, Yang H, Chao L
Forsythiae Fructus attenuates DSS-induced colitis and associated neuroinflammation with modulation of AMPK/mTOR-related autophagy signaling. Journal of ethnopharmacology | 2026-07-29
Forsythiae Fructus, the dried fruit of Forsythia suspensa (Thunb.) Vahl is a traditional herbal medicine widely used in East Asia for inflammatory disorders. Although Forsythiae Fructus exhibits anti-inflammatory activity in experimental colitis, its effects on colitis-associated brain inflammation and autophagy-related signaling remain unclear. This study investigated the protective effects of Forsythiae Fructus extract (FF) on intestinal and brain inflammatory responses in dextran sulfate sodium (DSS)-induced colitis mice and explored the involvement of AMPK/mTOR-related signaling. Mice received FF (100 mg/kg) or 5-aminosalicylic acid (ASA, 100 mg/kg) by oral gavage once daily for 15 days. DSS (5%, w/v) was administered in drinking water from day 7 to day 12, followed by a 3-day recovery period with normal drinking water (day 12-15). Disease severity, intestinal permeability, inflammatory mediators, and autophagy-related markers in the colon and brain were assessed using endoscopy, histology, ELISA, immunoblotting, immunofluorescence, and RT-qPCR. FF substantially alleviated DSS-induced colitis by attenuating body weight loss (-9.0% vs. -17.1% in DSS), reducing the disease activity index by approximately 40%, increasing colon length by 18%, and decreasing intestinal permeability by approximately 59%. FF restored epithelial barrier integrity by increasing Occludin, ZO-1, Muc2, and Tff3 expression. It also decreased IL-1β, IL-6, and TNF-α levels in the colon, serum, and brain, accompanied by reduced microglial activation and NF-κB signaling. FF increased AMPK phosphorylation and LC3B-II/LC3B-I ratios while reducing mTOR activation and SQSTM1 accumulation in both colon and brain tissues. FF effectively alleviated DSS-induced colitis, reducing disease activity by approximately 40% and restoring intestinal barrier function. These protective effects were accompanied by suppression of intestinal and brain inflammatory responses and modulation of AMPK/mTOR-related autophagy signaling. These findings provide experimental support for the traditional use of FF in inflammatory disorders and highlight its potential as a protective candidate for ulcerative colitis and its associated gut-brain inflammatory manifestations.
Park YJ, Pak ME, Yang HJ, Jin HJ, Kim KY, Hwang YH, Li W, Go Y
Citrullination of cathepsin H promotes NETs formation and exacerbates IBD via PI3K-Akt pathway.★ Cell reports | 2026-07-28
Peptidyl arginine deiminase 4 (PAD4) is previously known for its role in inflammatory bowel disease (IBD) through its facilitation of neutrophil extracellular traps (NETs) by citrullinating histones. However, the specific citrullinated substrates have not been fully elucidated, especially non-histones. By performing citrullination mapping, we unraveled the involvement of cathepsin H (CTSH), a novel substrate of PAD4, which undergoes citrullination at the R315 site. Then the citrullination of CTSH obviously altered its molecular conformation and subsequently reduced its enzymatic activity, which significantly boosted the formation of NETs. Consistently, CTSH knockout mice demonstrated exacerbated colonic inflammation and higher levels of NETs, which might be achieved by activating the phosphatidylinositol 3-kinase/protein kinase B (PI3K-Akt) signaling pathway. These findings underscore the critical role of CTSH in IBD pathogenesis and position it as a potential therapeutic target, highlighting the complex interplay among PAD4, CTSH, and IBD.
Song YH, Huang FX, Gu L, Chang X, Yang XY, Pang RX, Wu HC, Kang ZC, Li ZS, Bai Y
Switching from sulphasalazine or oral 5-aminosalicylic acid to another oral 5-aminosalicylic acid drug in the maintenance of remission in ulcerative colitis. The Cochrane database of systematic reviews | 2026-07-27
This is a protocol for a Cochrane Review (intervention). The objectives are as follows: To assess the probability of failure to maintain clinical remission, endoscopic remission, or both, following a switch from SASP or oral 5-ASA drug (comparator) to another oral 5-ASA drug (experimental) in adult ulcerative colitis patients at 52 weeks of follow-up. The intervention of switching to the experimental drug will be compared to the continuation of the comparator drug. To assess the safety of switching from SASP or oral 5-ASA to another oral 5-ASA drug in the aforementioned population.
Abed O, Hallan A, Norlén MM, Koch Hansen L, Munk Lauridsen M, Jørgensen MT, Kjeldsen J
Structural Characteristics and Superior Ameliorative Effects of Low-Molecular-Weight Homogalacturonan Compared with Rhamnogalacturonan-I from Avicennia marina Fruit Pericarp on DSS-Induced Colitis. Journal of agricultural and food chemistry | 2026-07-26
Pectic polysaccharides hold therapeutic potential for ulcerative colitis (UC). This study reports the first isolation of two structurally distinct pectins from Avicennia marina fruit pericarp: AMPP-2-1 (158 kDa), a rhamnogalacturonan-I (RG-I)-rich pectin with galactan branches and intricate arabinan side chains rich in β-Araf terminals; and AMPP-2-2 (16 kDa), a low-molecular-weight homogalacturonan (HG)-rich pectin with unsaturated GalpA at the nonreducing ends. Both pectins significantly ameliorated dextran sodium sulfate-induced UC by suppressing inflammation, restoring intestinal barrier integrity, and modulating gut microbiota to enrich beneficial bacteria while depleting pathogenic bacteria, alongside promoting short-chain fatty acid production. Low-molecular-weight HG showed greater ameliorative effects than RG-I under the present experimental conditions. These findings establish that pectins may contribute, at least in part, to the intestinal benefits of A. marina fruits in traditional use, expanding the structural diversity and biomedical applications of pectic polysaccharides from underexplored plant resources.
Li W, Huang Y, Su H, Nong J, Liang W, Liu Y, Zhao L, Yuan Q
Benzoylpaeoniflorin regulates macrophage polarization via the RNF31-DPEP2 axis to ameliorate intestinal mucosal barrier damage in ulcerative colitis. International immunopharmacology | 2026-07-26
Targeting macrophage polarization to restore immunological balance is a promising treatment strategy for ulcerative colitis (UC). This study aims to explore the preventive effects of benzoylpaeoniflorin (BPF) for UC and to elucidate the underlying mechanisms. Dextran sulfate sodium (DSS) was used to induce UC in mice, and BPF was administered simultaneously. Lipopolysaccharide (LPS)-stimulated RAW264.7 cells were used to model M1 macrophage polarization skewing, with BPF treatment applied. BPF improved DSS-induced colitis in mice, reduced M1 macrophage polarization, but significantly promoted M2 macrophage polarization in colonic tissues. After clearing macrophages in UC mice using clodronate disodium liposomes, BPF failed to further ameliorate UC progression in DSS + Mø-/- mice, indicating that macrophages are required for the protective effects of BPF against UC. Proteomics and in vitro/in vivo experiments further revealed that LPS treatment downregulated dipeptidase-2 (DPEP2) expression, while BPF treatment upregulated it. The promoting effect of BPF on DPEP2 expression is achieved by targeting RING finger protein 31 (RNF31) to hinder the binding of RNF31 to DPEP2, thereby inhibiting the ubiquitination and degradation of DPEP2 mediated by RNF31, and inhibiting the activation of the NF-κB signaling pathway. Moreover, DPEP2 knockdown or RNF31 overexpression neutralized the promoting effect of BPF on M2 polarization and its inhibitory effect on M1 polarization. Notably, BPF’s therapeutic benefits in UC mice were abolished by DPEP2 knockdown. BPF regulates macrophage polarization by modulating the RNF31-DPEP2-NF-κB axis, thereby ameliorating intestinal mucosal barrier damage in UC.
Yang Z, Li K, Li X, Zhong P, Hu Y, Yao X
Autophagy prevents ER stress-induced Tight Junction barrier disruption via claudin-2 homeostasis. bioRxiv : the preprint server for biology | 2026-07-20
Defective intestinal epithelial tight junction (TJ) barrier function and endoplasmic reticulum (ER) stress are central pathological features of inflammatory bowel disease (IBD), yet the molecular mechanisms ER stress to TJ disruption remains poorly understood. Here, we investigated the role of autophagy in regulating intestinal TJ homeostasis during ER stress. ER stress was elevated in inflamed Crohn’s disease tissue and chronic dextran sulfate sodium (DSS) colitis. In human intestinal epithelial Caco-2 monolayers, murine colon, and human colonic explants, induction of ER stress with tunicamycin, thapsigargin, or brefeldin A disrupted TJ barrier integrity, as demonstrated by reduced transepithelial electrical resistance and increased paracellular permeability. ER stress selectively increased the pore-forming TJ protein claudin-2 and altered occludin localization without significantly affecting other claudins. Pharmacologic activation of autophagy with rapamycin attenuated ER stress, restored TJ barrier function, reduced claudin-2 accumulation, and preserved occludin localization. Conversely, CRISPR-Cas9-mediated deletion of autophagy gene ATG7 exacerbated ER stress, apoptosis, and TJ barrier dysfunction in vitro, while intestinal epithelial-specific Atg7 knockout mice exhibited enhanced ER stress-induced intestinal permeability in-vivo. Mechanistically, prolonged ER stress impaired autophagic flux through IRE1α kinase signaling, resulting in accumulation of p62 and claudin-2. Inhibition of IRE1α kinase activity restored autophagy, reduced claudin-2 levels, and preserved TJ barrier function. We further identified adaptor-associated kinase 1 (AAK1) as a downstream mediator of IRE1α signaling during ER stress, with increased AP2M1 phosphorylation and altered claudin-2 trafficking. Claudin-2 overexpression alone induced ER stress and lysosomal damage, suggesting a feed-forward mechanism amplifying epithelial injury. Finally, enteric rapamycin administration reduced ER stress and restored autophagy in murine DSS colitis. Collectively, these findings identify an IRE1α-AAK1-autophagy axis as a critical regulator of intestinal TJ barrier integrity during ER stress.
Arumugam P, Saha K, Subramenium Ganapathy A, Wang A, Harris L, Yochum G, Nighot P
Protective effects of Brassica rapa L. water extract against DSS-induced acute UC-like colitis in mice and its regulatory mechanisms involving gut microbiota and the intestinal mucosal barrier. Frontiers in microbiology | 2026-07-13
The present study aimed to evaluate the protective effects of Brassica rapa L. (Br) water extract against dextran sulfate sodium (DSS)-induced acute ulcerative colitis (UC)-like injury in mice and to explore the underlying mechanisms. A DSS-induced acute UC-like colitis mouse model was established to assess the effects of Br administration. Disease severity was evaluated based on body weight loss, disease activity index (DAI) scores, colon length, colon weight, intestinal barrier integrity, and histopathological changes using H&E staining. Inflammatory mediators, TLR4/TLR9 expression, tight junction (TJ) proteins, gut microbiota composition by 16S rRNA sequencing, and intestinal metabolic profiles by UPLC-MS/MS-based non-targeted metabolomics were also analyzed. Br administration significantly ameliorated disease severity, as evidenced by mitigated body weight loss, reduced disease activity index (DAI) scores, attenuated colon shortening, normalized colon weight, and improved intestinal barrier integrity. Histopathological analysis (H&E) demonstrated that Br alleviated colonic tissue damage and inflammatory cell infiltration. The treatment also decreased the levels of proinflammatory mediators (IL-6, MPO, CXCL-1, and TNF-α) and downregulated the colonic expression of TLR4 and TLR9, while upregulating the expression of tight junction (TJ) proteins Occludin (OCC) and ZO-1. Furthermore, 16S rRNA sequencing revealed that Br restored gut microbial diversity and composition, specifically enriching potentially beneficial genera such as Alloprevotella, Lachnospiraceae_unclassified, and Alistipes, while suppressing the expansion of genera such as HT002. UPLC-MS/MS-based non-targeted metabolomic analysis suggested that Br was associated with the modulation of intestinal metabolic profiles, including changes in several putatively annotated metabolite features such as 12-Hydroxy-12-octadecanoylcarnitine and Vanillin. Br water extract alleviates DSS-induced acute UC-like colitis injury in mice, possibly by attenuating inflammatory responses, downregulating abnormal TLR4/TLR9 expression, improving intestinal mucosal barrier function, and modulating gut microbiota composition and associated metabolic profiles.
Wu J, Zhu X, Mao X
Cimicifuga foetida L. polysaccharide alleviates ulcerative colitis by inhibiting pyroptosis and regulating gut microbiota. Frontiers in pharmacology | 2026-07-13
Cimicifuga foetida L. is widely applied in the clinical treatment of ulcerative colitis (UC); however, its active components and mechanisms have not been deeply investigated. The objective of this study is to investigate the potential bioactive constituents of C. foetida L. for the treatment of UC, and elucidate its therapeutic mechanism. The crude polysaccharide of C. foetida L. was extracted by hot water and purified by DEAE Sepharose™ Fast Flow column to obtain, and named SM05. The structure was determined by HPLC, FT-IR and SEM. The effect of polysaccharide (SM05) on the mouse UC model and its mechanism of action were investigated using a dextran sodium sulfate (DSS)-induced UC model. Changes in body weight, disease activity index, colon length, organ index, histopathological injury, cytokine expression and intestinal tight junction proteins were measured to evaluate the effect of SM05 on UC. IHC, RT-qPCR, and 16s rDNA sequencing were performed to elucidate the underlying mechanism. SM05 is mainly composed of mannose, glucose, galactose, and arabinose. SM05 exerts antioxidant effects by activating the Nrf2/Keap1 pathway, thereby inhibiting the NLRP3-induced pyroptosis pathway. This reduces abnormal intestinal cell death and the secretion of inflammatory cytokines, thus protecting the intestinal barrier and suppressing further inflammation. Additionally, SM05 modulates the gut microbiota structure in mice with ulcerative colitis by reducing pathogenic bacteria (e.g., Bacteroides and Desulfovibrio) that damage the intestinal barrier and increasing the abundance of beneficial bacteria (e.g., Akkermansia and Saccharibacteria), thereby alleviating the progression of ulcerative colitis. In the preliminary biological assessment, the polysaccharide subfraction SM05 alleviated the symptoms of UC induced by DSS. This effect may be related to the activation of the Nrf2/Keap1 pathway, the inhibition of pyroptosis, and the regulation of the intestinal microbiota.
Luo Q, Xu Y, Li Z, Wang X, Cao L, Dong G, Guo S, Dai W
Microbiome & Immunology (4 papers)
Jianpi Bushen Qingchang Huashi formula alleviates DSS-induced colitis through butyrate-associated HDAC1 inhibition and Th17/Treg homeostasis. Journal of ethnopharmacology | 2026-07-29
Jianpi Bushen Qingchang Huashi Formula (JBQHF) is a traditional Chinese medicine compound of nine herbal ingredients clinically used to treat chronic diarrhea and dysentery syndromes, corresponding to ulcerative colitis (UC). Although clinical evidence supports its efficacy, the underlying mechanism remains unclear. This study sought to define the therapeutic benefit of JBQHF in a murine colitis model and to dissect the underlying mode of action. Ultra-high performance liquid chromatography coupled with quadrupole time-of-flight mass spectrometry (UHPLC-QTOF-MS) was applied to profile the chemical constituents of JBQHF. Therapeutic efficacy was evaluated in a DSS-induced murine colitis model. Gut bacterial composition and metabolite output were analyzed by 16S rRNA gene sequencing and Gas chromatography-mass spectrometry (GC-MS), respectively. Network pharmacology, deep learning-based virtual screening, and molecular docking were employed to predict candidate active compounds and their potential targets. Immunological assays focused on Histone deacetylase 1 (HDAC1) expression, HDAC enzymatic activity, histone acetylation status and the T helper 17/regulatory T (Th17/Treg) differentiation axis. JBQHF attenuated colitis as reflected by lower disease activity indices (DAI) and reduced histopathologic injury. Pro-inflammatory mediators were decreased while intestinal tight junction protein levels were elevated. JBQHF was associated with increased gut microbiota-derived butyrate production, reduced colonic HDAC1 expression and HDAC enzymatic activity, elevated Acetyl-H3K9 and Acetyl-H3K27, and a rebalancing of the Th17/Treg ratio. The protective effects of JBQHF were largely abrogated by the HDAC activator ITSA-1. Deep learning-based virtual screening further identified flavonoids within JBQHF as candidate HDAC1 ligands with predicted target selectivity. JBQHF ameliorates experimental colitis via a dual inhibition of HDAC1, providing an integrated mechanism for its clinical application.
Feng W, Wang Y, Jin Z, Chen J, Li B, Xu S, Jing X, Lu Y, Dai S, Ge L
Scleroglucan ameliorates dextran sulfate sodium-induced ulcerative colitis and gut microbiota dysbiosis in mice.★ International journal of biological macromolecules | 2026-07-25
β-1,3/1,6-Glucans exhibit significant potential as therapeutic agents for ulcerative colitis (UC); nevertheless, most existing studies have focused on yeast β-glucans. In the current research, we assessed the therapeutic effects of scleroglucan (SCL), a β-1,3/1,6-glucan produced from the fungus Sclerotium rolfsii, by using a dextran sulfate sodium (DSS)-induced mouse model. SCL treatment significantly attenuated DSS-induced body weight loss from 18.45% to 14.69%, reduced the disease activity index from 3.83 to 3.11, decreased colonic TNF-α and MPO levels, and restored IL-10 concentrations (p < 0.05). SCL also promoted goblet cell proliferation and upregulated Muc2 gene expression (p < 0.05), but had no significant effects on colon length and tight junction proteins. Additionally, SCL significantly increased cecal acetate to 10.82 μmol/g, propionate to 3.87 μmol/g, butyrate to 7.13 μmol/g, and valerate to 1.16 μmol/g, compared with the respective levels of 3.11, 1.61, 1.67, and 0.60 μmol/g in the DSS group. Consistently, enhanced colonic mRNA expression of GPR41, GPR43, and GPR109A was seen with the SCL group than the DSS group (p < 0.05). SCL also remodeled gut microbiota composition, and significantly elevated Bacteroidetes, Lactobacillus and Ruminococcus, and reduced Firmicutes (p < 0.05), a microbial profile associated with attenuated colitis severity. Taken together, these findings indicate that SCL effectively mitigated DSS-induced colitis, emphasizing its potential as a bioactive polysaccharide for developing functional foods to assist UC nutritional intervention.
Zhao Y, Wen Y, Yin D, Yang F, Zhong Y, Hu J
Poricoic acid a ameliorates ulcerative colitis via AMPK/PPARγ pathway-dependent cellular senescence inhibition and concomitant gut microbiota-metabolome modulation.★ Phytomedicine : international journal of phytotherapy and phytopharmacology | 2026-07-22
Ulcerative colitis (UC) is an intractable inflammatory bowel disorder characterized by persistent intestinal inflammation and impaired gut barrier integrity. Its pathogenesis is multifactorial, involving gut microbiota dysbiosis, metabolic dysfunction, and cellular senescence. Current therapeutic regimens remain limited, underscoring an urgent need for innovative agents that target these interrelated pathological cascades. This study aimed to evaluate the pharmacological effects of poricoic acid A (PAA) on DSS-induced senescence in intestinal epithelial cells and in a murine model of ulcerative colitis (UC), as well as the underlying molecular mechanisms. We established a DSS-stimulated senescent intestinal epithelial cell model and a DSS-induced UC mouse model. Multi-omics and bioinformatics strategies, including network pharmacology, transcriptome profiling, gut metagenomics, and intestinal targeted metabolomics, were combined with molecular docking to predict candidate signaling axes. Subsequent pharmacological inhibition and siRNA-mediated silencing assays were performed to validate core pathways functionally. PAA robustly suppressed DSS-induced senescence and inflammatory responses in intestinal epithelial cells. In vivo assays verified that PAA alleviated UC-related manifestations, including body weight loss, rectal hemorrhage, and colonic histological injury. Joint network pharmacology and transcriptomic screening identified the AMPK/PPARγ as the core pathway mediating PAA’s bioactivity. Mechanistic experiments confirmed that PAA directly bound and activated PPAR, further functionally triggering downstream AMPK/SirT1/PGC1α signaling. Blockade of AMPK via pharmaceutical antagonists or siRNA largely abolished PAA’s anti-senescence and anti-inflammatory capacities; PPARγ suppression, in turn, secondary deactivated the AMPK and its downstream functional effectors. In mouse models, AMPK inhibition drastically compromised PAA’s protective effects against UC. Moreover, PAA treatment of UC is closely associated with remodeling of the gut microbiome-metabolome axis and restoration of intestinal homeostasis. PAA exerts potent anti-senescence, anti-inflammatory, and colon-protective effects in UC via activating the AMPK/PPARγ signaling pathway. Such beneficial activity may be associated with the normalization of gut microbiota-metabolome homeostasis. This work identifies novel molecular targets and a promising lead compound for the intervention of ulcerative colitis.
Wang Y, Liu Z, Hou Q, Xu Y, Chen W, Chen M, Liu J, Tang J, Wang Y, Zhou M
Epithelial Chloride and Bicarbonate Transport in Intestinal Barrier Failure: A Molecular Target-Validation Assessment of CFTR and SLC26A3/DRA in Inflammatory Bowel Disease.Review International journal of molecular sciences | 2026-07-17
Current inflammatory bowel disease (IBD) therapies suppress immune pathways, yet epithelial recovery can remain incomplete. This review evaluates whether intestinal chloride and bicarbonate transport can support a distinct, adjunctive pharmacological strategy. Rather than cataloguing transport proteins, we compare the cystic fibrosis transmembrane conductance regulator (CFTR), SLC26A3/down-regulated in adenoma (DRA), and TMEM16A/ANO1 against an evidence hierarchy of human disease relevance, causal epithelial biology, pharmacological tractability, target engagement, functional rescue, and developability. CFTR and DRA form the most coherent module linking bicarbonate availability to mucin expansion, epithelial surface pH, fluid balance, and barrier organization, but their liabilities differ. CFTR is structurally and clinically druggable, yet its modulators are genotype-directed, and broad activation may worsen diarrhea. DRA has stronger evidence for a colonic barrier role and emerging support from human organoids, but no validated activator or stabilizer. TMEM16A has abundant chemical tools, yet uncertain selectivity, wide extra-epithelial expression, and no established disease-modifying role in IBD. No intervention has achieved mucosal healing through anion-transport rescue in IBD. We therefore define the decisive experiments required before translation: confirmation of persistent functional defects in human tissue, selective exposure-linked rescue in patient-derived epithelium, direct target engagement, and protection against hypersecretion or electrolyte imbalance. The evidence supports focused, mechanism-based evaluation of the CFTR-DRA axis rather than empirical repurposing.
Seo Y
Biomarkers & Precision Medicine (1 papers)
Mechanism and Active ingredients of Gancao Qinlian Granules in ameliorating ulcerative colitis:integrated in vivo, in vitro, network pharmacology and untargeted metabolomics investigation. Journal of ethnopharmacology | 2026-08-01
Gancao Qinlian Granules (GQG) are a granulated formulation of the classical prescription Gancao Xiexin Tang, originally documented by Zhang Zhongjing in the Treatise on Febrile and Miscellaneous Diseases (Shang Han Za Bing Lun, c. 220 CE). This formula comprises six medicinal components: Glycyrrhiza glabra L. (Gancao), the radix of Scutellaria baicalensis Georgi (Huangqin), Ziziphus jujuba Mill. (Dazao), the rhizomes of Zingiber officinale Roscoe (Ganjiang), the dried tuber of Pinellia ternata (Thunb.) Breit (Banxia) , and the rhizoma of Coptis chinensis Franch (Huanglian). GQG has been extensively employed in traditional and contemporary clinical practice for the treatment of ulcerative colitis (UC). Nevertheless, its candidate bioactive constituents and underlying mechanisms of action remain incompletely elucidated. To comprehensively characterize the chemical composition of GQG and elucidate its therapeutic mechanisms against UC through an integrated strategy combining network pharmacology prediction, serum/colon/fecal multi-omics profiling (metabolomics and microbiome), and experimental validation. Initially, GQG was analyzed by UHPLC-Q-Exactive Orbitrap MS under negative/positive ion modes, with compound identification via mzCloud, HMDB, and literature matching. C57BL/6 mice (n=8/group) were induced with UC using 3% dextran sulfate sodium (DSS) for 15 days. UC-related targets from GeneCard, PharmGkb, TTD, and OMIM were integrated to construct compound-target-pathway networks (Cytoscape 3.10.1). Secondly, GQG (9g/kg/d, 12g/kg/d, 15g/kg/d) or mesalazine (300 mg/kg) was administered orally for 10 days. Disease severity was assessed daily via Disease Activity Index (DAI: weight loss, stool consistency, bleeding). Post-euthanasia, colon length was measured, and histopathology (H&E, Alcian Blue-Periodic Acid Schiff staining) analyzed mucosal damage and goblet cell depletion. Colon IL-1β levels were quantified by immunohistochemistry (IHC). Then, serum, fecal, and colonic tissue samples underwent UHPLC-Q-Exactive Orbitrap MS-based untargeted metabolomics. Differentially expressed metabolites (DEMs) were identified (VIP >1, p<0.05) and pathways enriched via KEGG. Fecal 16S rDNA sequencing (Illumina NovaSeq) analyzed microbial α/β-diversity and differential taxa (LEfSe, LDA score >3). Subsequently, Integrated component analysis, network pharmacology, and metabolomics data to obtain the mechanism by which GQG improves UC, and verify the related target proteins through IHC and Western blot. Finally, obtain the candidate bioactive constituents in GQG through molecular docking, and verify the efficacy of these bioactive constituents with their targets on a cellular model. Chemical profiling revealed 121 constituents in GQG, with 53 flavonoids (43.8%) including core bioactive markers (e.g., licoflavone B, licuroside). In DSS-induced ulcerative colitis mice, GQG (12g/kg/d) exerted potent therapeutic effects: reducing disease activity index, attenuating colon shortening, restoring goblet cells, and suppressing colon IL-1β. Mechanistically, GQG remodeled gut microbiota composition and function, increasing beneficial taxa (Muribaculaceae, Lactobacillus). This microbiota restructuring directly drove metabolic reprogramming. Suppression of pro-inflammatory metabolism: purine degradation (hypoxanthine), tryptophan-derived uremic toxins (kynurenine), pathogenic bile acids (deoxycholic acid). Integrative analysis of the microbiota-metabolite axis reveals that GQG extract can regulate the NF-κB/NLRP3 inflammasome cascade through p-NF-κB p65 expression, NLRP3 assembly (NLRP3, Caspase-1), and ASC speck formation. Combined with molecular docking, six key components in GQG exhibit high affinity for critical targets. In vitro cellular experiments demonstrate that these core candidate bioactive components effectively inhibit key targets within the target pathway. GQG ameliorates UC by modulating gut microbiota structure and function, restoring microbial co-metabolism (e.g., SCFA synthesis, bile acid homeostasis), and subsequently inhibiting the NF-κB/NLRP3 inflammasome axis. This integrated approach substantiates the ethnopharmacological application of GQG for UC.
Liao G, Zhu M, Zhang Y, Zhai S, Chen C, Yan Z, Fu L, Zheng L, Song C, Yu Y
IBD-associated Neoplasia (1 papers)
A Case of Adenocarcinoma in a Stoma Site after 27 Years of Stoma Surgery for Hirschsprung’s Disease.Case report Surgical case reports | 2026-07-24
Adenocarcinomas originating at stoma sites are extremely rare. While many cases are associated with colorectal cancer or inflammatory bowel disease, instances without such predisposing factors are even rarer. A 39-year-old man with a history of Hirschsprung’s disease presented with tumor growth at his permanent stoma site, which had been established 27 years earlier. A biopsy confirmed adenocarcinoma. Preoperative imaging, including CT, MRI, and PET-CT, showed no evidence of lymph node or distant metastasis. Immunohistochemical staining (CK7+, CK20+, CDX2+) was consistent with a primary tumor of the small bowel. Based on the preoperative diagnosis of localized disease and the clinical goal of preserving intestinal function, local resection was performed with negative margins. Histopathological examination confirmed a primary ileal adenocarcinoma. The patient remains recurrence-free 30 months postoperatively without adjuvant chemotherapy. This report presents a rare case of stoma-site adenocarcinoma arising 27 years after surgery for Hirschsprung’s disease. In long-term survivors of pediatric stoma surgery, chronic physical and chemical irritation may contribute to malignancy even in the absence of a predisposing malignant background. Malignancy at the stoma site can be discovered by patients through self-examination; therefore, both patients and clinicians must recognize the potential risk for early detection.
Koro D, Shonaka T, Tani C, Takeda T, Otani M, Ohara M, Hayashi T, Kamikokura Y, Aoki N, Tanino M
Category Distribution
TipWant More Control?
The Interactive Dashboard lets you filter and search across all categories, download results as CSV or Excel, and explore the full 30-day backlog - useful if you missed a week or want to search by keyword across a wider date range.
Subscribe via RSS to get daily updates automatically, or use the per-category feeds to follow just one subfield.